|
A. Introduction Type-C retroviruses have long been implicated in the etiology of leukemia and lymphoma in various animal species. Animal models exist for exogenous, horizontal, transmission of these naturally occurring RNA tumor viruses in animals and are especially well characterized for cat, cow, and some other species [21]. Human T-cellleukemia-lymphoma virus (HTL V) is the first type-C retrovirus consistently isolated and associated with specific human malignancies. It is distinct from prcviously identified animal retroviruses by molccular [15] and immunologic studies [10, 16, 17]. It is an exogenous virus that must be acquired by infection (i.e., not transmitted in the germ line), since HTLV proviral sequences are present in DNA of neoplastic T cells, but not in DNA of nonneoplastic B cells from the same patient [7] or in normal tissues [15]. In this report we summarize clinical and epidemiologic features which suggest that HTL V is etiologically linked to certain malignancies. Our data demonstrate that HTL V is associated with cases of mature T -cell leukemia-Iymphoma with common clinica] features. These cases tend to cluster in a restricted distribution whcrc HTL V infection is prevalent. Occasional paticnts from virus nonendemic areas probably acquired HTL V infection prior to developing their T -cell leukemia-lymphoma through travel into HTL V endemic areas and close contact with residents in these areas. B. Materials and Methods Samples from various patient and normal populations were submitted as frozen or lyophilized serum or plasma. The clinical and pathologic diagnoses were as recorded by the submitting investigator except for certain cases where pathologic material was reviewed by one of us (E.J.). Serum antibodies to a disrupted whole virus preparation were detected by a modification to thc technique previously reported [14]. Natural antibody to the major core protein p24 of HTL V was detected by a radioimmune precipitation (RIP) as previously described [9]. C. Clinical and Pathologic Features The majority of cases from which HTL V has been isolated, or in
which HTL V antibodies have been detected, share many common features.
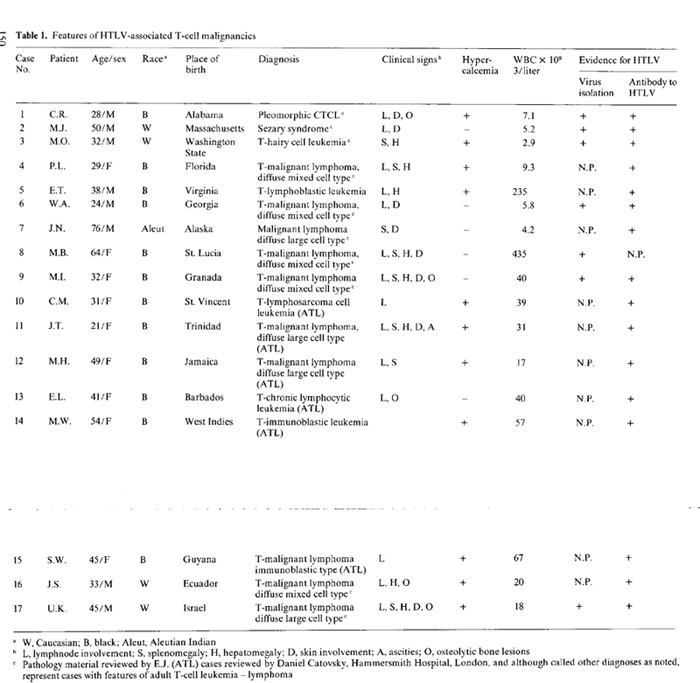
Summarized in Table I are the clinica] and pathologic characteristics
of HTL V -positive cases from the Western Hemisphere and elsewhere
( details of HTL V -positive cases from Japan are not included in
this report). In all cases in the series, and in cases from Japan
[II, 18], HTLV has an association with lymphoma or leukemia of mature
differentiated T cells. In current immunopathologic nomenclature,
the broad category of malignancies of mature T cells includes T
-cell chronic lymphocytic leukemia, cutaneous T -cell lymphomas
(CTCL) (mycosis fungoideslSezary syndrome), peripheral T -cell lymphoma,
lymphosarcoma cell leukemia (T -LCL), and adult T -cell ]eukcmia-Iym
phoma (A TL). As shown in Table I, HTL V is most commonly associated
with peripheral T -celllymphomas (classification in the working
formulation [ I] as large cell, diffuse mixed, or immunoblastic
cell type), TLCL, and A TL. Although two of these 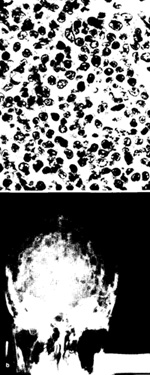
cases were classified as CTCL, this association is rare since they
are the only two out of over 200 cases from the United States, England,
and western Europe that were positive for HTL V serum antibodies.
As is evident from Table I, the histopathologic diagnoses given
vary considerably. There are, however, certain morphologic features
shared by most of these tumors. The tissues show diffuse proliferation
of a pleomorphic population of lymphoid cells (Fig. I a). The cells
tend to vary considerably both in size and shape. In most cases,
cells from all points in the spectrum are present in equal proportions,
and such cases are designated as diffuse, mixed cell type by both
the Rappaport classification and the working formulation [I]. In
other cases, one large lymphoid cell type predominates, and such
cases are designated as diffusc large cell, or diffuse large cell,
immunoblastic lymphoma, based on the characteristics of the proliferating
cells. An inflammatory background is normally not evident. The histopathologic
features described above are similar to those seen with certain
other peripheral T -cell lymphomas not associated with HTL V. Thus,
there are no specific pathologic features that can be recognized
at this point as indicating an HTL V -associated leukemia/lymphoma.
Similarly, there is quite a spectrum in the clinical presentation
of cases, which may present a.s lymphoma, leukemia, or lymphoma
with leukemic involvement. Some cases appear associated with fulminant
and rapidly progressive disease, whereas others have a much more
indolent and chronic clinical course. Thus, the exact relationship
of HTLV to a specific clinical entity is far from established. Therefore,
systematic surveys in HTL V -endemic and nonendemic areas, with
special attention to precise immunologic classification of malignant
cells, will be needed to clarify thesc relationships further. In
addition the recent observation ofantibody-negative, antigen-positive
cases of CTCL (C. Saxinger, personal communication) point to a need
for caution in defining virus-disease relationships. Ultimately
"molecular" epidemiologic studies of defIned disease categories
will need to be undertaken before final conclusions can be drawn.
D. Disease Associations and Case Clusters To evaluate the relationship of HTL V infection and disease, sera
from over 900 cases of adult and childhood malignancies from diverse
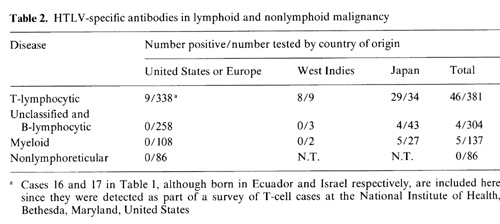
geographic areas have been tested for HTL V antibodies [6]. As shown
in Table 2, only 55 of 914 were positive. None of the nonlymphoreticular
neoplasms were positive, indicating that HTL Vis probably trophic
tor cells of thc Iymphoreticular compartment. The bulk of the positives
were from patients with dcfinitc T -cell malignancies. The remaining
nine were from patients with lymphoid and/or myeloid leukemias from
Japan. Since some of these cases come from the viral endemic area
and/or in some cases have been extensively transfused, the etiologic
significance of this association remains to be established. HTL
V is most closely associatcd with A TL diagnosed in Japan, and 29
of the 34 patients in this series were positivc [6]. Among cases
ofT -Cell non-Hodgkin's lymphoma (T -NHL), 6 of 12 from Japan were
also positive. These positive T -NHL cases appear to share featurcs
with cases from the United States and elsewhere as recorded in Table
I. The eight cases of HTLVpositive A TL from the Caribbean region
(cases 8-15 in Table I in this series) confirm the propensity for
geographic clusters of HTL V -associated cases to share clinical
and pathologic features [2,4]. Studies of normal populations providc
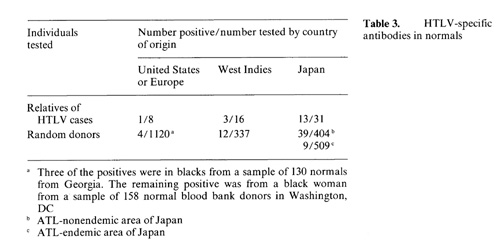
a model for examining the role of HTL Vas an etiologic agent. The
detection of HTL V antibodies in relatives of cases is of interest
since it may reflect the infectivity ofHTLV. In Table 3 we summarize
the data on members in nine families of HTL V -positivc malignancies.
Excpt for one family from Japan in which four of eight members were
antibody positive, in all other cascs only one first-degree relative
was found to be positive. The fact that both spouses and blood relatives
were positive leads us to suspect horizontal rather than vertical
E. HTLV Infection and Adult T -cell Malignancy The frustrating failures of virologists in the past to demonstrate and isolate a uniquely human type-C RNA tumor virus etiologically linked with leukemia or lymphoma has led to the belief that retroviruses play no rolc in these or other human malignancies. Human T -cell leukemia-lymphoma virus (HTLV) is the first human virus of this class consistently identified in association with a specific type of human leukemia-lymphoma [5, 12, 13]. The epidemiologic data summarized here demonstrate that HTL V is associated with several malignancies of the T cell, but not solid tumors or other hematopoietic tumors [6]. Although the role of HTL Vas an etiologic agent is not established, it is striking that the distribution of cases is limited to a relatively narrow spectrum of mature T -cell leukemia-lymphoma cases with common features. In further support of the notion that HTL V and T -cell leukemia-lymphoma are related is the limited distribution of HTL V infection in the general population. Although most dramatic in Japan, where HTL V seropositivity appears geographically associated with clusters of A TL [ II, 18], a similar pattern is emerging in the Caribbean [2, 4] and more recently in the southeastern United States blacks [3]. In two cases from the United States (case 2, MJ, case 3, M.O.) both the clinical and epidemiologic features were distinct from the bulk of other cases. Both patients, how ever, had histories of travel to and close contact with persons in viral endemic areas. These exceptions to the rule provide further evidence for a virus-disease relationship since it is likely that their HTL V infection was acquired in viral endemic regions. Studies of migrants into HTL V endemic regions may prove especially informative in further delineating etiologic relationships. In summary, we postulate that HTLV, unlike other putative tumor viruses, is not widespread in distribution but rather is limited to certain regions of the world and within limited areas of some countries (e.g., southwestern Japan). In at least three areas, Japan, the Caribbean, and the southeastern United States, HTL V -associated disease is a mature adult T -cell leukemia-Iymphoma. Identification of cases in some other areas of the world suggests that a similar pattern of virus prevalence and disease occurrence will emerge. Thus, although further studies will be needed to establish a causal relationship, the story thus far is similar to that of the retrovirus association with leukemialymphoma in animals in which satisfaction of Koch's postulates has established an etiologic role for C-type retroviruses. References I. Berard CW, Greene MH, Jaffe ES, Magrath I, Ziegler J (1981)
A multidisciplinary approach to non-Hodgkins lymphomas. Ann Int
Med 94:218-235 |